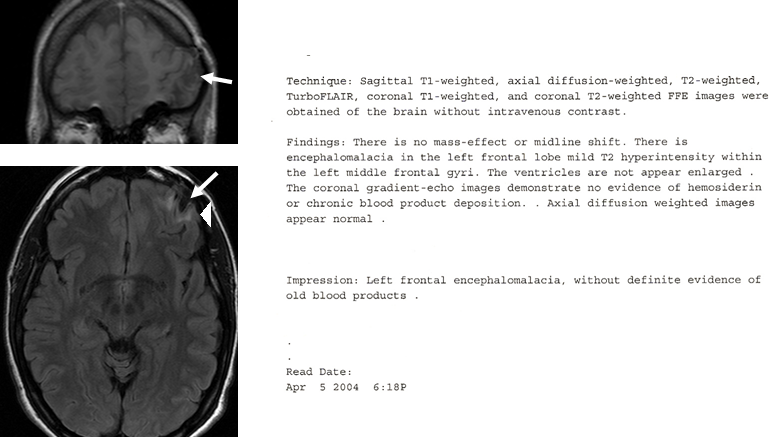
| The result came as a shock to JS: Encephalomalacia in the left frontal lobe
and mild T2 hyperintensity within the left middle frontal gyri. These anomalies
were minor but consequential. They partly (if not fully) accounted for the
behavioral anomalies that had prompted this imaging investigation. In the
following years, JS received social security support, first in Minnesota, later
in California (where she had spent most of her childhood and part of her
youth). |
| Unable to decide on her further living, JS began to travel the world.
Although mentally handicapped, she was able to profit from high cognitive
aptitudes and skills. Grown-up as a bilingual (English & Hebrew), she
easily acquired further languages: French, Portuguese, and starting with 2006
German. In 2006, we met in Vienna (Austria). At that time I was in charge to
organize in Austria the International ‘Brain Awareness Week’ of the ‘Dana
Alliance for the Brain’. JS found us in a DANA magazine and on the internet and
offered to donate her brain for research purposes. Insecure how to react to
such a sinister offer, we replied that at least we would have to wait for her
death… When she arrived at Vienna (to learn German, as she said), I quickly
found out that she was not about to die so soon at all. As a brain researcher,
I became interested in her case. I was perplexed by this coexistence of a
highly functional personality with subtle behavioral defects that become apparent
only upon closer attention. JS asked me to explain to others, what kind of
defects these are. This is the reason for this text. |
| So: what kind of mental defects JS is suffering from? To understand these
defects, we need to delve into the functional architecture of the human brain. This
is the most complicated of our organs, nevertheless great advances have been
made in the exploration of its functioning, also thanks to the careful
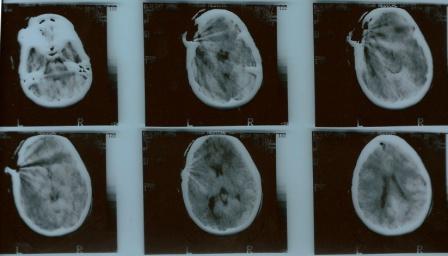
observation of cases like JS. What exactly happened to JS’s brain on February
25th in 1984, when the car she was in on the back bench left the
road so unduly and fell 10 m into a ditch? The medical exposé of the Rambam
Medical Center in Haifa where the victim was rushed to reads as follows: |
| Deep wound on left forehead, from eyebrow to parietal area, pulsing dura
exposed, subdural air. Operated under general anesthesia, small tear in dura,
minimal contusion below. Wound closed without reconstruction of skull defect.
Superficial consciousness for 2½ days. Release after 8 days, no overt
neurological deficits. |
| This last remark stirred hopes in the family that JS, then 9½ years old and
such a beautiful and charming girl, would have been lucky and would recover
fully from this severe incident. But the neurosurgeon should have known better.
He had seen pieces of broken bone, subdural air, and the small tear in the
dura. These observations leave little doubt that the injury had affected not
only the skull but also the brain tissue below. And behind the eyebrow lies the
orbitofrontal cortex, getting its name by its tight contact with the orbit, the
bony cavity harboring the eye. It is no surprise that another deficit remaining
from this injury was a partial loss of eyesight on the left side. |
| The orbitofrontal cortex belongs to the ‘prefrontal cortex’, the ‘pre-‘
indicating that this area lies ahead of those frontal areas that are
responsible for our motor and sensory functions. Lesions to one of these
anterior regions have no overt consequences on motoric or sensory functions. On
first glance, the patient may appear unaffected. A famous historic example is Phineas
Gage who in 1848 lost his left eye and parts of his left prefrontal cortex at
the age of 25 during a working accident. Against the common narrative that Mr.
Gage after the incident had turned from a decent gentleman into a bad-mannered,
hard drinking and highly unreliable villain, the injured recovered
astonishingly well, serving for 8 years a demanding job as a long-distance
stagecoach driver in Chile. The injury of JS is much smaller and more
localized. The accident did not result in a loss of brain tissue, but
disconnected parts of the left orbitofrontal cortex from its regular
addressees. Which connections have been affected in detail cannot be told from
the structural MRI scan. In addition, we still do not fully understand all
functions of the human orbitofrontal cortices (furthermore, the left and the
right one seem to serve slightly differing tasks). As a preliminary working
hypothesis, the neuroanatomical position of these gyri suggests a role in
connecting the prefrontal cortex to the so-called ‘limbic system’. |
| The different parts of the prefrontal cortex occupy the highest level in
cerebral information processing, not under direct sensory or endocrine influence.
Their genuine task seems to consist in overseeing and coordinating lower level
activities. Therefore, they are often said to harbor our reason. Since the
orbitofrontal cortex sustains connections to the limbic system mostly dealing
with emotions like joy, anger, fear, sadness and disgust, it is assumed that
this high level area somehow integrates our feelings into reasonable thinking.
Thanks to reasonable thinking, we can resist impulses telling us to immediately
follow our actual spontaneous inclinations. For example, it will be wise to
treat our neighbor politely, then he will probably be helpful if we get in
trouble. Reason acts with foresight and is able to withhold the reasonable from
giving way to attractions leading to transient rewards with unfavorable long-term
consequences. The most important addressee in the limbic system for the
orbitofrontal cortex seems to be the amygdala. The most prominent feeling
elicited by amygdalar activity is fear. Undisturbed interplay between the
amygdala and the orbitofrontal cortex informs our reason about the emotional
(negative) value of a fearful face. If this interplay is handicapped, the
afflicted has difficulties to attach emotional value to impressions that
normally would be classified as fearful. Social learning is at the heart of our
behavioral development. Children strongly depend in their habit formation on
social feedback. They have to interpret continuously social cues as positive or
negative, disclosed to them often in casual and informal settings. Smooth
interplay between the prefrontal cortex and the limbic system provided, these
social interactions will occur without much effort or the need to pay focused
attention to them. |
| Having laid out these – in part still speculative – neurobiological
background, we might now be in the position to understand, how a rather limited
lesion in the left orbitofrontal cortex should lead to difficulties to comply
with social norms. If the lesion occurred at some later stage of development
(as in the case of JS at the age of 9½ years), many basic habits have already
formed. They probably will persist although it is not totally clear to which
extent their persistence depends on the continued input of information. On the
other hand, many habits typically acquired only during puberty and early
adulthood will be much more difficult to form. It will not be sufficient simply
to see an angry face as guidance into the complex realm of dos and don’ts. New
habits in compliance with social norms will only form upon patient and often
repeated explanation and logical argument. We cannot take the easy way from the
limbic system to reason, going by the amygdala and the orbitofrontal cortex.
This path is not fully operating in JS’s left hemisphere. If others understand
some social relationships and facts of increasing complexity by a simple, less
than friendly glance, JS needs the full program: proof or disproof, detailed
material, majority and minority opinion, examples, exceptions, and so forth. For
her social contacts, this disposition may in the long term be tiresome and
irritating. Probably she will have problems making friends, but more sincere
friends may appreciate her serious and diligent approach to matters of sometimes
daunting complexity. She has no fear of complexity, even if surrounded by warning
social cues. The prefrontal cortical areas in JS’s brain are very well in the
position to fulfil their internal functions, even if one of them is not working
well. Sometimes, it may even be of advantage if the ‘traffic between reason and
feelings’ is not running so smoothly. Then, the intact rest of the prefrontal
cortex can deal with matters without being disturbed by emotions (which all too
often are of transient or even redundant significance). This sometimes allows JS
to accomplish impressive feats requiring a high level of deliberation and
synthesis. |
| Let’s have Brita a final word on JS, a sincere friend during her time at St. Olaf sharing a room with her back in
the 90ies (the comment is from June 06): |
| “…her priorities and the
way she thought about things were unique… She particularly had trouble with
authority figures when she conflicted with them… I also noticed that she would
learn in unique ways as well. She excelled in anything that required
memorization or detail oriented work, but things that required integration of
information was baffling to her. I remember talking to her about a French class
we were taking together. She was having a very difficult time reading a book in
French because she would have to stop and define every single word that she
didn’t know. She was unable to figure them out from the context, or get the
gist of the story even though her vocabulary was far above average. … She is
exceedingly logical and has a hard time identifying or understanding her
emotional world. Everything must be explained and explored to a great degree
before she is comfortable with it. …” |